CMS has repeatedly kicked the can down the road concerning Liability Medicare Set-Asides guidelines and how to protect Medicare’s future interest in an injury case. Even though Medicare has not issued any guidelines for Liability cases as they have for workers’ compensation cases, the same Medicare Secondary Payer (MSP) statute that applies to workers’ compensation cases also applies to liability cases. Plaintiff attorneys should understand the risks when Medicare’s interest is not considered.
Below is a list of the 5 plans deemed primary to Medicare by the statute:
-
- Workers’ Compensation
- Auto
- Liability
- No Fault
- Self-Insured Plans
There is a common misconception that the need to protect Medicare’s future interest in a case is limited to workers’ compensation claims. It is important to understand the risks associated with not addressing Medicare’s interests in a liability settlement for a Medicare beneficiary. While there is no official guidance on how to address Medicare’s future interest in a liability case, the lack of guidance does not mean that the MSP statute no longer applies.
How Will Medicare Find Out About My Case?
In December 2009, Congress passed the Medicare and Medicaid SCHIP Extension Act that requires primary payors (insurance carriers, TPAs, etc.) to first determine if an individual whose case is settling is a Medicare beneficiary. The primary payer must then report the “required information,” once the case is resolved, to the Secretary of the Department of Health and Human Services in the “form, manner, and frequency” the Secretary prescribes. Failure to do so can result in civil monetary penalties of up to $1000 per day, per claim. This information includes over 200 data fields related to the case, including ICD-9 and ICD-10 codes, accident/injury descriptions, parties involved in the settlement, and personal identifying information for the plaintiff. Once this information is received by Medicare, they place a marker in their system that helps them track and deny case-related treatment and prescriptions. This forces the individual to use their settlement funds for future treatment related to the case. If those funds are spent per Medicare’s guidelines and they become exhausted, Medicare will step in as the primary payor going forward.
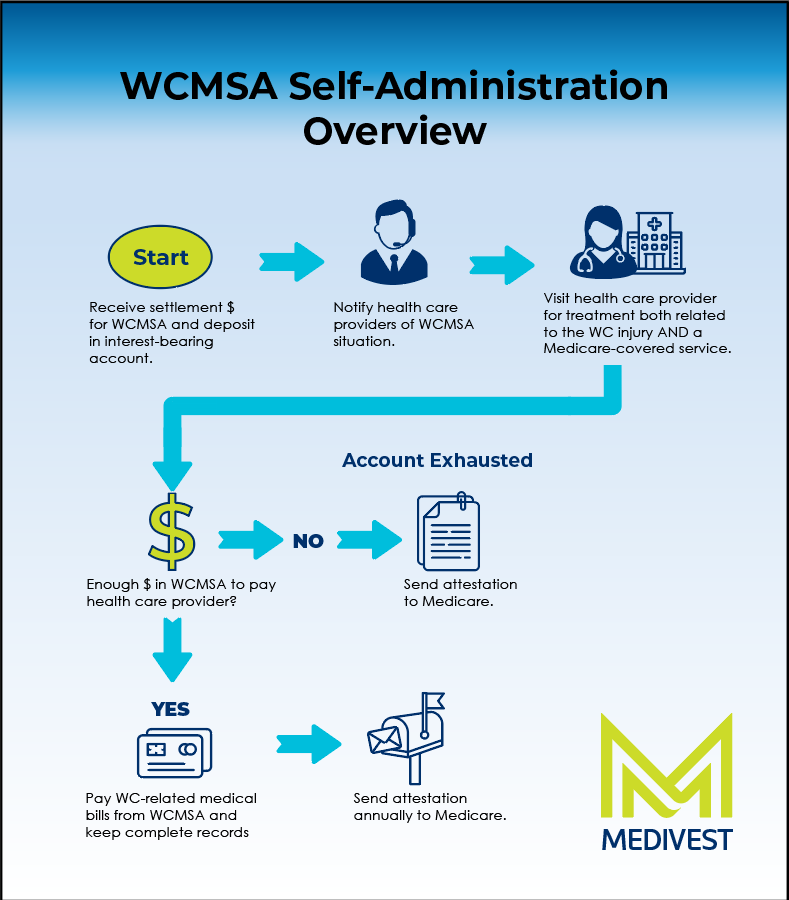
With the increased oversight for cases involving a Medicare beneficiary, steps must be taken to protect Medicare’s past and future interests in the case. While there is no statute in place that requires a Medicare-Set-Aside (MSA) arrangement in workers’ compensation or liability cases, it is one of the few methods that have been proven to address Medicare’s concerns.
Determining if a Medicare Set-Aside (MSA) arrangement is the right choice for your case depends on several factors
-
- Is the individual currently receiving Medicare benefits or will be receiving Medicare benefits within the next 30 months?
- Is the individual over 62.5 years old?
- Is the individual currently receiving Social Security Disability Insurance (SSDI) or has an open application for SSDI benefits?
- Is there a need for Medicare-covered, case-related treatment, and prescriptions based on the medical records?
If the individual meets the criteria listed above, a Medicare Set-Aside is the most conservative method available to comply with the MSP statute with respect to Medicare’s future interest in the case. The Medicare Secondary Payor Statute gives Medicare rights as a secondary payor, and they are prohibited from making a payment when there is a primary payor involved. Failure to address Medicare’s interest in the case typically results in Medicare denying payment for Medicare-covered, case-related treatment and prescriptions. If a MSA amount is not designated as part of the settlement, CMS has indicated they can assume the net settlement amount to the individual is the “future medical fund” and they will not step in to pay for case Medicare-covered, case-related treatment and prescriptions until all the funds are spent according to Medicare’s guidelines for MSA funds. Designating a MSA amount establishes a paper trail of what was done to protect Medicare in the settlement, and it will limit Medicare from considering the entire net settlement amount to the individual to be the MSA amount.
If the MSP statute is ignored during the settlement process, Medicare can deny payment for Medicare-covered, case-related treatment and prescriptions until documentation is provided showing how much out of the settlement was set aside and how those funds were spent. Designating a MSA amount allows you to set aside a piece of the pie. By not designating a MSA amount, the individual may be required to spend all of their net settlement funds on Medicare-covered, case-related treatment before Medicare agrees to step in and become the primary payor again. CMS would require proof that the funds were spent correctly before doing so. It is much better to set aside a piece of the pie than the whole pie.
As you work toward settlement, it is important to understand how addressing Medicare compliance issues creates a safety net for individuals, should their condition deteriorate over time. Medicare’s primary mechanism to enforce the MSP statute is a denial of payments. If settlement funds have not been spent by Medicare guidelines for MSA funds, Medicare will deny payments leaving the individual in a bad situation. Even though CMS has not issued guidelines for liability settlements, the MSP Statute of 1980 clearly states that liability is a primary plan, and you must protect Medicare’s interest in the case.
In the end, the greatest risk lies in doing nothing. By taking a conservative approach and preparing a Medicare Set-Aside, you help protect all parties and ensure compliance every step of the way.
About Medivest
Founded in 1996, Medivest is a national Medicare Secondary Payer (MSP) compliance company and provider of settlement solutions. Our focus is assisting anyone settling a workers’ compensation or personal injury claim to understand their obligation to consider Medicare’s interests under federal law. Medivest provides pre- and post-settlement solutions that help mitigate exposure from that obligation. Contact us today at 877-725-2467 or medivest.com/contact-us.