U.S. Supreme Court Fires a Shot at CMS by Overturning the Chevron Deference Case
In Loper Bright Enterprises v. Raimondo, No. 22-1219, 2024 WL 3208360 (U.S. June 28, 2024), the U.S. Supreme Court has reinstated the power of federal courts to interpret federal statutes over agency interpretations of same. While courts have always deferred to agency determinations of fact (for example, demand amounts for repayment of MSP conditional payment liens, denial of payment of medical items, services or expenses by Medicare, or denial of waiver requests by Medicare for repayment of MSP debt for which the four step administrative appeals process before seeking redress in federal District Court has existed), this case signals more power being placed in the hands of the federal judiciary with respect to interpretations of law. It specifically places the power to interpret laws that Congress has enacted into the hands of the federal courts.
The Medicare Secondary Payer Statute originally enacted in 1980 and found at 42 U.S.C. Section 1395y(b)(2) (MSP) is a federal law placing Medicare as a secondary payer to other insurance called primary plans including liability, self-insurance, No Fault, and Workers’ Compensation plans when a primary plan has demonstrated an obligation to pay via judgment, settlement, payment, or other arrangement. The MSP on its face gives Medicare the right to recover any injury related payments (conditional payments) without regard to the timing of the payment. The Centers for Medicare & Medicaid Services (CMS), the sub agency of the Department of Health and Human Services, is the regulatory agency in charge of administering the Medicare program. Since the enactment of the MSP, CMS has promulgated regulations under the Code of Federal Regulations that have helped implement the MSP.
MSP Enforcement Has Been Focused on Recovery of Conditional Payments up to Date of Settlement
Despite the definition of conditional payments not being limited to dates of service prior to the Date of Settlement, enforcement for the recovery of conditional payments by CMS has been focused on recovery of conditional payments made by Medicare for dates of service from the Date of Injury up to the Date of Settlement. CMS has also written guidance interpreting the MSP, early on in the form of memos and more recently, in the form of the Workers’ Compensation Medicare Set-Aside Arrangement Reference Guide (WCMSA Reference Guide) which incorporates any of CMS’ prior memos it wanted to still be referred to WCMSA Reference Guide v4.0 April 2024.
Often heard by those in the MSP Compliance industry and from CMS at various conferences is the concept that parties are to consider Medicare’s interests in any settlement. The consideration of Medicare’s past interests in any settlement has always been relatively straightforward, with the need for attorneys representing injured parties and the need for primary plan payers to confirm whether Medicare made any injury related payments, and once auditing any payment summaries to confirm injury relation, to pay the proper amount and/or request compromises or waivers for same so that any Medicare lien is addressed at the time or prior to settlement.
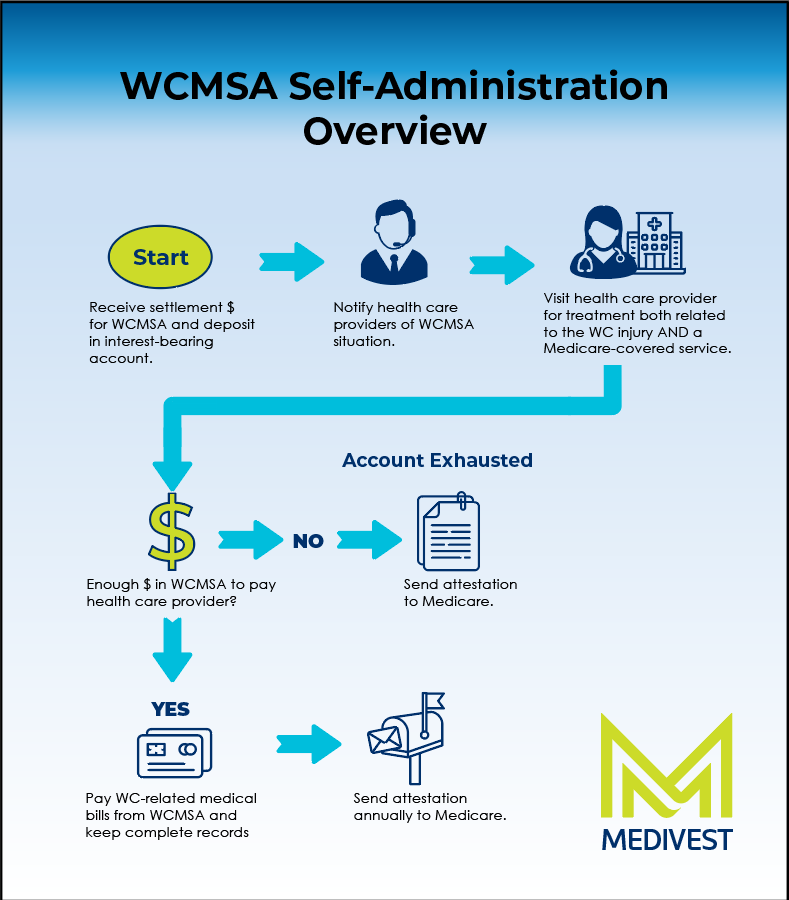
What has been more uncertain is whether and how to address Medicare’s future interests in settlements for any primary plan settlement. The area where Medicare Set-Aside allocation reports and the administration of same is most often encountered is in the Workers’ Compensation arena. The WCMSA Reference Guide has become the predominant standard espoused by CMS to protect Medicare’s future interests in Workers’ Compensation settlements that meet CMS’ workload review threshold requirements (for current Medicare beneficiaries, settlements of over $25,000 or for those who have a reasonable expectation of becoming enrolled in Medicare within 30 months of settlements over $250,000, CMS allows a WCMSA allocation report to be reviewed for adequacy)
We have written about the attempts of CMS to promulgate regulations on how Medicare beneficiaries should protect Medicare’s future interest in liability settlements but how on two occasions (most recently in 2022), CMS has withdrawn its intent to address how to adequately protect these Medicare future medicals in liability cases via regulation. Some have speculated that instead of the more formal regulation process, CMS would either update its WCMSA Reference Guide or write a new version specific to liability settlements.
In the absence of specific regulations or guidance, it has been up to the risk tolerance of settling parties in the liability realm to analyze and evaluate best practices to consider Medicare’s future interests, and decide whether to put aside some dollars as a version of a Medicare Set-Aside in liability settlements when the MSP law clearly puts Medicare as a secondary payer to the liability settlement funds used to compensate future medicals, but in light of the various factors that make liability settlements different from Workers’ Compensation and No Fault settlements. We have discussed the differences between types of settlements before, but the main differences are that liability settlements are often constrained by policy limits, may have reductions in payment due to varying degrees of comparative negligence, may include payments for derivative claims of family members (loss of consortium for a spouse or loss of companionship of a minor child as examples), and include a variety of non-economic damages that do not compensate for medicals (Pain and Suffering and Loss of Enjoyment of Life as examples).
Take Aways
Interestingly, this Loper Bright Enterprises case could give rise to a federal court’s interpretation of protection of Medicare’s future interests in a settlement in a way different from CMS’s operational interpretation to only collect conditional payments up to the date of settlement in liability cases. This means there could be a time in the future when more liability plaintiffs will choose to request liability Medicare Set-Aside allocation reports (LMSA’s) from entities that perform medical reviews and analyze the amount, if any should be set aside to protect Medicare’s future interests in light of the unique factors of their case. This means plaintiffs’ attorneys will need to give their clients adequate information to allow for informed consent regarding this Medicare futures issue. While many WC carriers and claimants choose to establish Medicare Set-Asides for use in paying injury related medicals instead of shifting the burden of payment onto Medicare, a lower percentage of injured plaintiffs (or the carriers insuring liability defendants) choose to do the same. Could this decision mean a decision is imminent on how settling parties shall consider Medicare’s future interests in liability settlements? Probably not, but the framework is set for a federal court to take on the issue.
Will this mean that CMS guidance is of no use or that courts won’t read agency guidance? No. However, it does signal a pendulum swing away from a regulatory agency like CMS with more power placed back into the hands of the courts. It is also a warning to Congress to get it right because if a statute is not clear on its face, there seems to be more power placed with the courts to interpret how to implement and how to interpret federal statutes like the MSP.